How far are we from full closed-loop?
Apr 07, 2026
ATTD2026 is over. The data has been presented, the slides have been shared, the conversations have moved from lecture halls to corridors, to dinners, to quiet reflections on the flight back home.
And one question keeps coming back.
Are we there yet?
Not in terms of innovation. Not in terms of ambition.
But in terms of reality—for the person sitting at the dinner table, looking at their plate, still wondering:
“Do I need to bolus for this?”
The dream we are all chasing
For decades, diabetes care has been built around one central burden: anticipation.
Anticipating meals.
Anticipating glucose rises.
Anticipating mistakes.
Full closed-loop promises something radically different: removing anticipation from the equation.
“The best technology is not the one that adds more control.
It’s the one that removes the need for it.”
And yet—removing boluses is not trivial. It is, in many ways, the hardest problem in diabetes technology.
Meals are unpredictable. Humans are unpredictable. Life is unpredictable.
And algorithms are trying to catch up.
A glimpse of the future: Medtronic (now MiniMed)
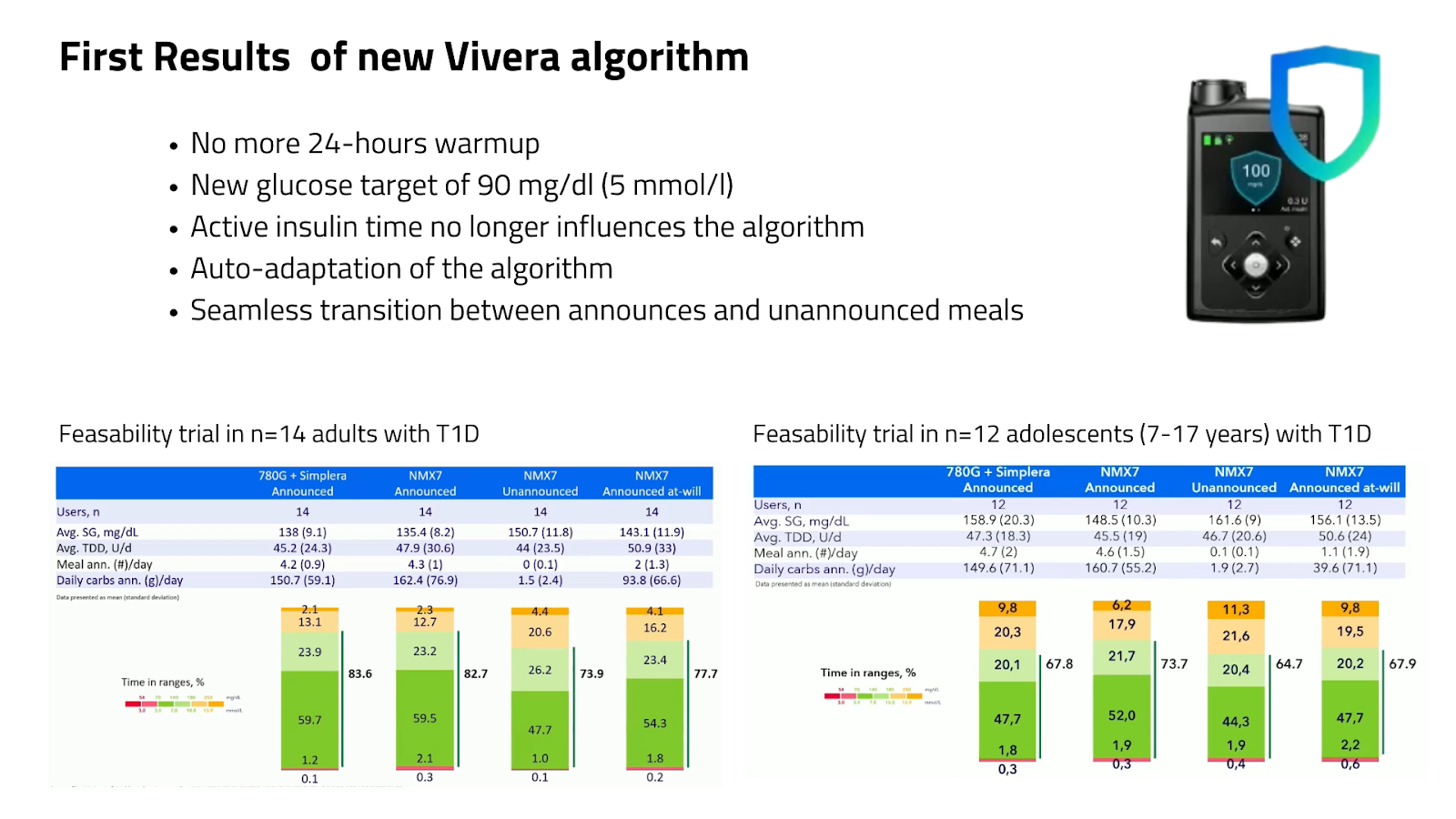
Images presented at ATTD2026
The first data on the new MiniMed full closed-loop algorithm felt like a quiet but important step forward.
Adults reached a TIR of 74% without bolusing. Adolescents around 65%.
That matters.
Because for the first time, we are seeing numbers that start to approach what we consider “clinically acceptable”—without asking the user to intervene.
But let’s be honest:
When people do bolus, current systems still perform better.
So we are not replacing hybrid closed-loop yet. It is a transition toward something simpler.
A system where people may achieve glycemic targets safely without announcing meals.
The road is still long—pivotal trials, regulatory approval, expected launch around 2027–2028 (subject to regulatory approval and local reimbursement criteria)..
But the direction is clear.
A different philosophy: Insulet
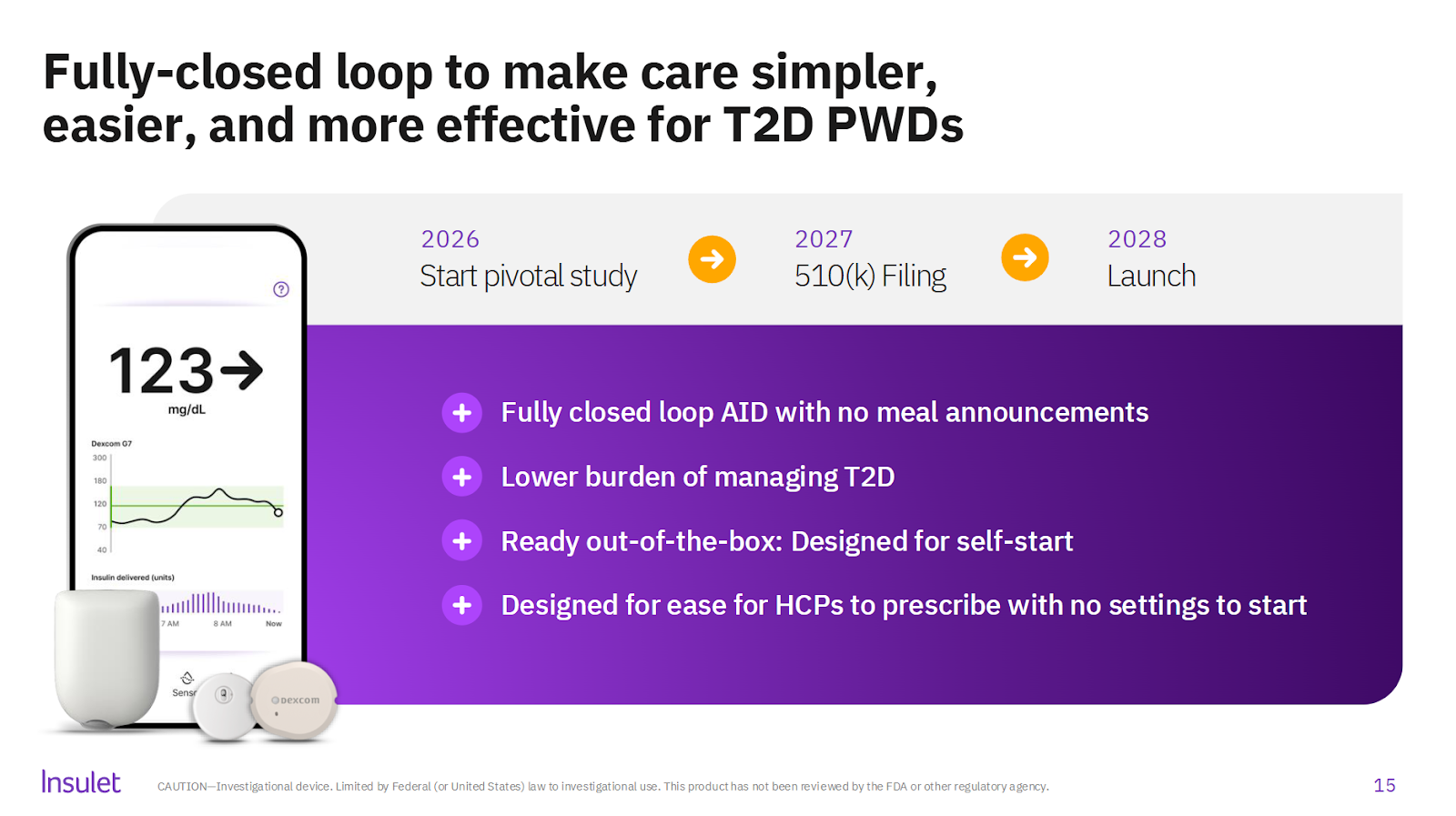
Slide > investor presentation Insulet Feb 2026
If MiniMed aims to reduce the burden of mealtimes while maintaining outcomes, Insulet is taking a more radical approach.
Not just fewer boluses.
No boluses. No settings. No decisions.
A system designed so that neither the patient nor the clinician needs to “manage” it.
In their Evolution studies—focused now on type 2 diabetes—we see TIR approaching 68% in people starting from higher HbA1c levels.
Not perfect. But that’s not the point.
The point is accessibility.
“Simplicity is the ultimate sophistication.” — Leonardo da Vinci
For millions of people with type 2 diabetes, the barrier is not the lack of technology.
It is the complexity of using it.
If Insulet succeeds, this could be one of the biggest shifts in diabetes care—not because it’s the most advanced system, but because it might be the most usable one.
The rise of intelligence: Tandem Diabetes Care
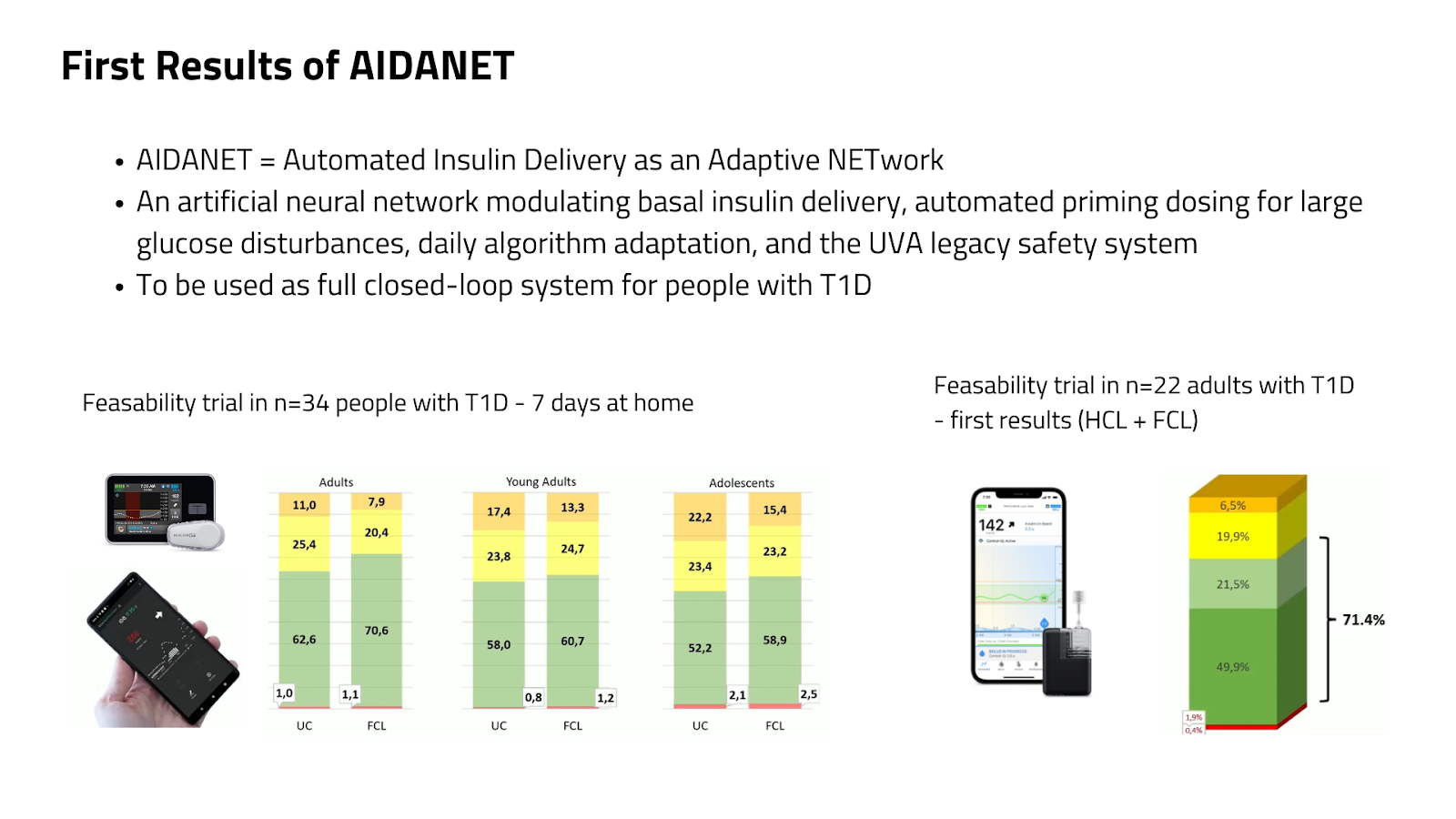
Images presented at ATTD2026
Tandem’s work tells a different story.
Not simplification—but intelligence.
Their Freedom algorithm shows what is currently possible: around 60% TIR without boluses. A starting point.
But the real signal comes from AIDANET—a neural-network-based system.
This is where things start to change.
Because traditional algorithms follow rules.
AI-based systems learn.
They adapt. They personalize. They evolve.
And early data already shows improvement over time.
“We are not programming the future anymore.
We are training it.”
The challenge now is no longer technical. It is regulatory.
First to arrive: Ypsomed / CamDiab
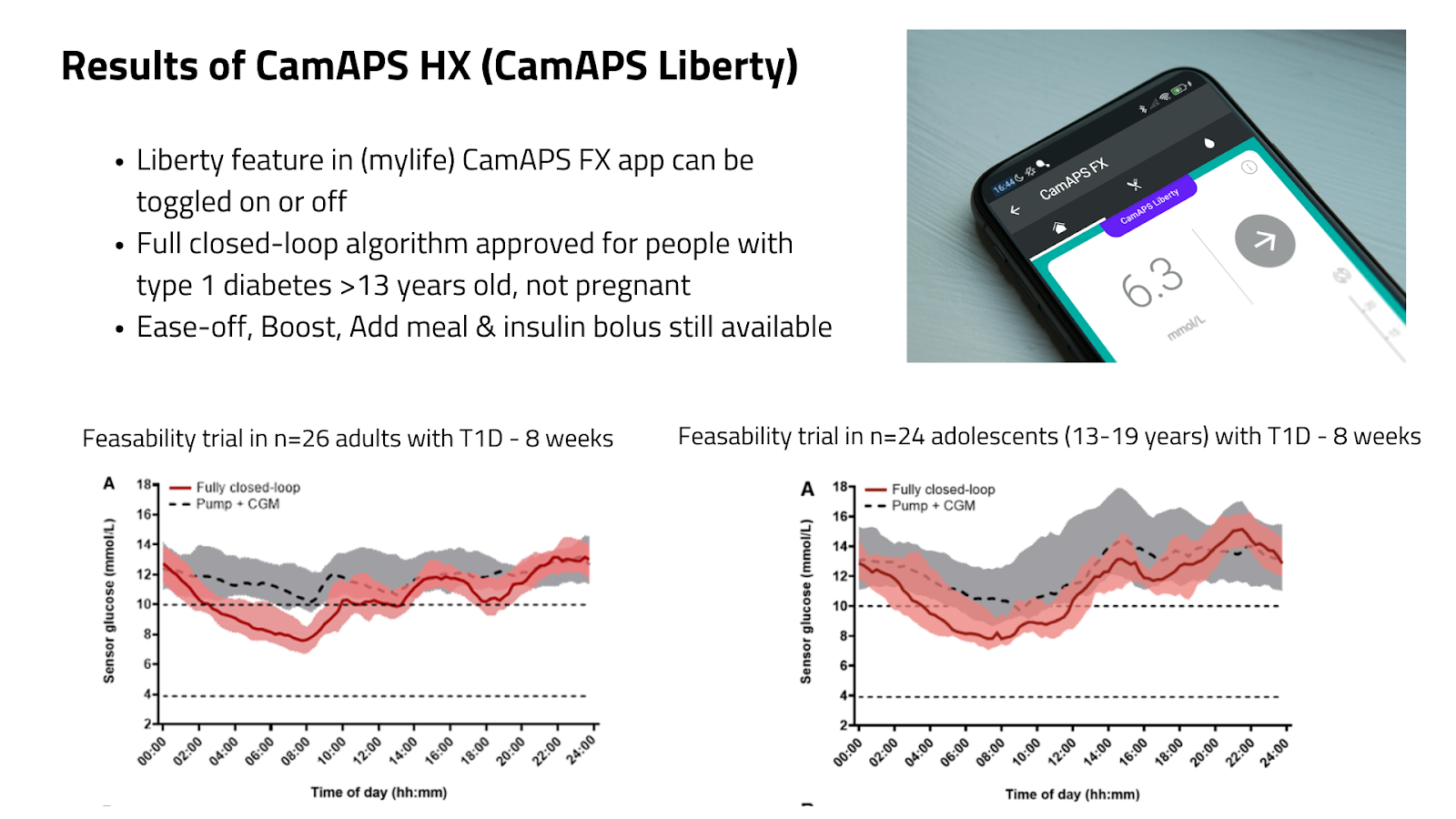
CamAPS HX may not be the most performant system (see results in adults and adolescents) — but it will likely be the first full closed-loop system people can actually use.
And that matters more than perfection.
Because real-world use teaches us more than controlled trials ever will.
The upcoming Liberty feature—allowing users to use the system without meal boluses—marks a turning point.
Not because it solves everything.
But because it gives people a choice.
“Progress doesn’t start with perfection.
It starts with permission.”
The unexpected shortcut
While engineers are refining algorithms, something else is happening quietly—but powerfully.
People are already stopping boluses.
Not because the system is perfect.
But because biology is being modified.
In the open-source world—especially with systems like AndroidAPS—we see increasing use of GLP-1 and GLP/GIP receptor agonists
Reducing post-meal spikes. Flattening glucose curves. Lowering insulin needs.
Even in type 1 diabetes.
Off-label—but widespread.
This is uncomfortable for some.
But it is real.
And it raises an important question:
What if full closed-loop doesn’t come from technology alone?
What if it is the combination of:
- smarter algorithms
- better sensors
- and adjunct therapies
that finally gets us there?
So—are we there yet?
No.
But we are closer than we’ve ever been.
And more importantly, we are asking better questions.
It is no longer: “Can we remove meal boluses?”
It is: “What level of control is acceptable if we do?”
Today:
- 70% TIR is considered good (American Diabetes Association)
- 80% is already emerging as the new standard (ISPAD)
Hybrid systems are approaching 80%.
Full closed-loop systems—today—are still around 60–70%.
That gap is the space we are working in.
Where this leaves us
For now, the advice does not change:
Yes, bolusing still improves outcomes.
Yes, carb counting still matters.
But something fundamental is shifting.
The burden is slowly moving—from the person to the system.
And maybe, in a few years, we will look back at meal bolusing the same way we look at urine glucose testing.
Necessary once.
Unimaginable now.
“The future arrives slowly… and then all at once.” — Ernest Hemingway
We are still in the “slowly” phase.
But not for long.
Hopeful.
Kind regards,
![]()