#ATTD2023: updates on AID systems
Mar 02, 2023
Welcome to this first comprehensive blog post about the ATTD2023!
In this post you'll get the latest updates on closed-loop systems discussed at the conference.
Read on to find out what updates there are for the
- MiniMed 780G,
- Tandem Control IQ,
- Omnipod 5,
- Diabeloop,
- CamAPS FX,
- INREDA,
- and Dexcom's new full closed-loop algorithm: Project Liberty!
PS: As a reminder, the following abbreviations are used:
- TIR = time in range = time between 70 -180 mg/dl or 3.9 - 10 mmol/l (goal in most people with diabetes: >70%)
- TBR = time below range = time < 70 mg/dl or 3.9 mmol/l (goal in most people with diabetes: <4%)
- GMI = Glucose Management Indicator = estimated HbA1c based on sensor data (goal in most people with diabetes: <7%)
- AID systems = Automatd Insulin Delivery systems (= closed-loop systems)
Get Access To Updated Diabetes Technology Courses
1. MiniMed 780G

Real-world data from 61 481 users of the MiniMed 780G

More and more people are using the MiniMed 780G, and the results from all those CareLink reports continue to be very good:
- the average TIR among >61 000 users worldwide is 73%,
- the TBR is only 1.7%,
- and the GMI 6.9%!
This makes the MiniMed 780G the only closed-loop system that can systematically demonstrate an average GMI <7% on such a large scale.
Please note: these are averages. Not everyone achieves a TIR of 73%....

Here you can see that half of the people (50%) on a MiniMed 780G do not achieve GMI <7%, TIR >70% ánd TBR <4%!
In fact, your glycemic control on an AID system also depends on:
- how well you were regulated before starting the AID system,
- your age (older people tend to do better than children and adolescents),
- the number of times you give an insulin bolus (with MiniMed 780G it was already shown that >4x/d boluses were associated with better results compared to fewer boluses)
- and your settings (with MiniMed 780G, it has already been shown that the best results are achieved with a target value of 100 mg/dl or 5.6 mmol/l and an active insulin time of 2 hours).
Trends in meal boluses among >61 000 MiniMed users

A lot of interesting things were noticed in this real-world data of >61 000 people, which also allows Medtronic to make some recommendations around the use of meal boluses.
Most people use a carbohydrate ratio of 10 g/E

Real-world data show that the carbohydrate ratio is set on average at 10 g/U.
- Among those >15 years of age, this was relatively stable at 5-10 g/U. Prof Cohan said that probably many people set the carbohydrate ratio at 10 g/U for convenience, and that he sometimes also did this. His suggestion was mainly not to make it too difficult.
- Among children ≤ 15 years of age, the average carbohydrate ratio was slightly higher, averaging 12.9 g/U, with slightly more variation within this group.
"Simplify, simplify, simplify or you could do as me: just pick 10 g/U" - prof Ohad Cohen
Fewer time blocks of carbohydrate ratio are sufficient (1-2 in adults and 2à3 in children)

If you look at the number of carbohydrate ratios used per day, you will see that on average only 2 carbohydrate ratios are used.
- For people >15 years, this averaged 1.9 carbohydrate ratios per day; for children ≤15 years, this averaged 2.4 carbohydrate ratios per day.
- The majority of people on MiniMed 780G use <2 carbohydrate ratios per day.

Further research by Medtronic shows there was no relationship between the number of carbohydrate ratios used per day and the TIR.
Therefore, the suggestion is to keep it simple here as well:
- 1-2 carbohydrate ratios for adults
- and 2-3 carbohydrate ratios per day for children are sufficient.
In children, adjust grams of carbohydrate input and carbohydrate ratio according to growth

What did stand out is that over time the mean TIR seems to drop, especially in children: -10.5% decline TIR in children ≤ 15 years over 12 months.

A cause was sought, and they believe it is due to not enough grams of carbohydrates being entered in the system and the carbohydrate ratio not being strengthened enough.
- Indeed, over 12 months, a progressive increase in the total insulin daily dose was seen, which is what you would expect in children who grow during one year.
- However, the amount of grams of carbohydrates per day remained stable, which you would not expect. Children who grow normally eat more.
- And the carbohydrate ratio also remained fairly stable, whereas you would expect it to strengthen (decrease) even more at 12 months.
Thus, in children, it is especially important to pay attention to correct input of grams of carbohydrates and correct setting of the carbohydrate ratio.
The amount of grams of carbohydrates per day over a year should increase, and the carbohydrate ratio over a year should strengthen (decrease) in accordance with physiological growth.
What if you don't bolust for a meal?
The MiniMed 780G seems to be safe in people who bolus very little, however this was at the expense of 10% TIR.
- In a study with 14 MiniMed 780G users, the TIR was shown to be 78% with 5.5 boluses per day, and 68% with 1.7 boluses per day.
Also shown was a study that looked at postprandial glycemia at meals with different carbohydrate portions, without bolusing.
- No significant difference was seen in postprandial glycemia after meals of ≤ 20 grams of carbohydrates. Thus, the MiniMed 780G is perfectly capable of accommodating this.
- A difference was seen at meals of > 20 grams though, which increased as you took in more carbohydrates.
- Meals up to 80 grams were tested, and no ketoacidosis or other problems were noted at any meal, suggesting that it is safe not to bolus for meals up to 80 grams.
No photos were allowed to be taken of either study; they were going to be published.
Thus, the conclusion here is that the fact that people who do not bolus before every meal should not be excluded for closed-loop systems.
This study (Akturk et al. DTT 2022) also reached the same conclusion with Tandem Control IQ.
What if you can't count carbs?

In a recently published study (Petrovski et al. Diabetes Care 2023, which was also discussed at ADA2022), fixed portions were shown to work almost as well as carb counting.
- The TIR with fixed servings ("fix meal management") was 74%,
- compared to a TIR of 80% with carb counting("flex meal management").
From this, it was decided that people who cannot count carbs should certainly not be excluded for this technology.
In other words, it is no longer necessary to be able to count carbs to qualify for the MiniMed 780G (or other closed-loop systems).
So, in general, closed-loop systems should be offered to anyone with type 1 diabetes,
even though that person may not be bolusing for every meal, or may not be able to count carbohydrates.
For a high-fat meal, it is sufficient to enter only the carbohydrates

Medtronic did a "pizza study" to see how best to handle a high-fat meal with the MiniMed 780G.
- To do this, they first had the exact number of carbohydrates, fats and proteins determined from 2 pieces of standard pizza.
- Then they had 15 adults with type 1 diabetes on the MiniMed 780G eat 2 pieces of standard pizza 9 Monday nights in a row:
- 3 x in manual mode with entry of carbohydrates only (TIR was then 65%, TBR 6%),
- 3 x in closed-loop with also entering carbohydrates only (TIR 86%, TBR 2.7%),
- and finally 3 times in closed-loop with a "fixed bolus" (TIR 78%, TBR 2.5%).
Again, the conclusion was that fixed boluses did almost as well as carbohydrate counting,
and that glycemic control was very good despite not taking into account fats and proteins.
Thus, with the MiniMed 780G, it is sufficient to enter only the carbohydrates (without taking fat and protein into account) during a high-fat meal.
When exercising, it is best to use a temporary target of 90 min before exercise and 25% less meal insulin

As for sports, a nice study was shown on different ways to handle sports with the MiniMed 780G.
- Dr McCarthy received 80,000 euros in funding to conduct this SMART study (Optimising glycemia around physical exercise with advanced hybrid closed-loop therapy use in type 1 diabetes).
- 10 people with type 1 diabetes on the MiniMed 780G did 3x 45 min of moderate-intensity exercise 90 min after breakfast.
- They set their insulin release in 3 different ways
- 100% bolus insulin and temporary target value at start of exercise,
- 25% reduction in bolus insulin and temporary target 90 minutes before exercise,
- and 25% reduction of bolus insulin and temporary target 45 minutes before exercise.

The main focus was on glycaemic control during to 105 minutes after exercise.
- If the full bolus insulin was given, and the temporary target only started at the start of sports, participants had as much as 34% TBR or hypoglycemia!
- In contrast, if bolus insulin was reduced by 25%, and the temporary target was used from 90 minutes before exercise, TBR was only 1.1%.
The latter strategy was thus able to avoid all sports-related hypoglycaemia here, and did so without increasing hyperglycaemia (TIR was 82% in this group).
What's next?

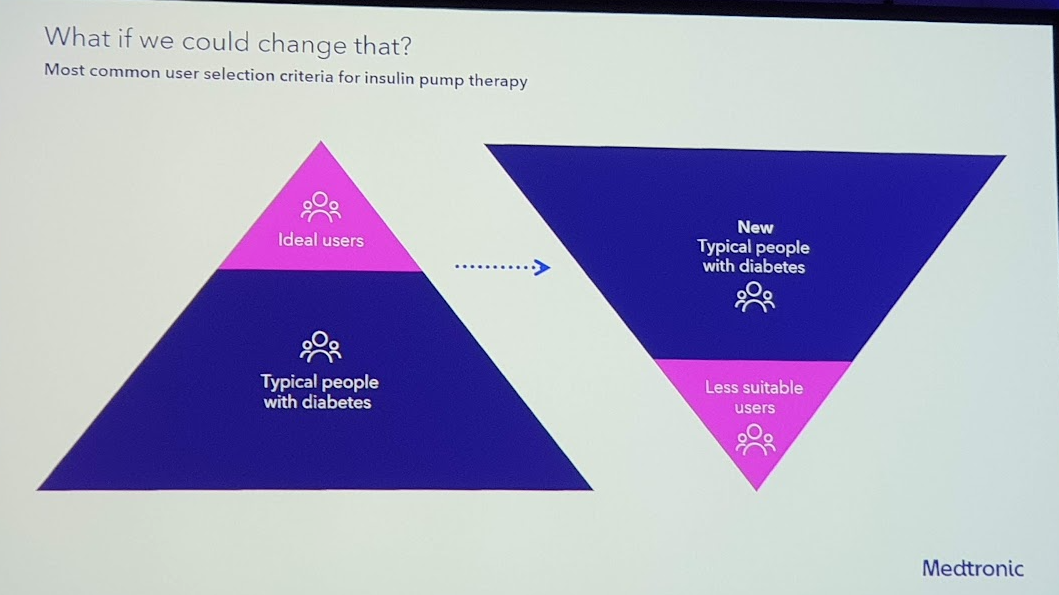
Instead of focusing on even better glycaemic control with TIR of 80-90%,
Medtronic's pipeline is mainly trying to make the system easier to use so that it is accessible to more people.
They plan to do this with
- automatic meal detection (in a session on their Klue technology, it appears that drinking movements could also be successfully integrated)
- and the easier Simplera CGM.
A timeline for these 2 updates was not given, but the promoslides are already there.

Finally, there are also rumours that Medtronic might buy Eoflow.
In that case, the SmartGuard algorithm will potentially become available with an EoPatch X pump, giving Medtronic a solid patch pump immediately...
2. Tandem Control IQ

According to Tandem's latest quarterly update, there are now as many as 420 000 people worldwide using a Tandem t:slim X2 pump.
It is estimated that 2/3 of these (280 000 people) also use Control IQ, making Tandem Control IQ the most widely used closed-loop system in the world
Effect from day 1

From a meta-analysis of the 3 "pivotal" randomised studies (n=369, ages 2-72) with Tandem Control IQ, the following conclusions were drawn, amog others:
- TIR increased from 57% to 70%, and HbA1c dropped from 7.5% to 7.0%,
- and the TIR increased from the first day Control IQ was used.
These data are similar to the larger real-word datasets:
- Breton et al. DTT 2021: data from 9451 people on Control IQ for 1 year
- Kovatchev et al. Diabetes Care 2022: data from >19 000 people on Control IQ for 3 months
Control IQ in type 2 diabetes
Currently, about 20 000 people are also said to be using Tandem Control IQ off-label in type 2 diabetes.
Tandem plans to apply for an official indication for this too.
- At ADA2022, real-world data were already shown that Tandem Control IQ has about the same effect in people with type 2 diabetes as with type 1 diabetes.
- At DTM2022, a prospective "feasibility study" showed Tandem Control IQ was safe and effective in 30 people with type 2 diabetes.
- A true pivotal study to obtain the indication will be planned in the near future.
At the ATTD2023, real-world data were shown from n=936 people with type 2 diabetes on Tandem Control IQ.
- These people had worn Basal IQ for a minimum of 1 month and then Control IQ for 3 months.
- 3 months after switching from Basal IQ to Control IQ, the TIR increased from 63% to 71%.
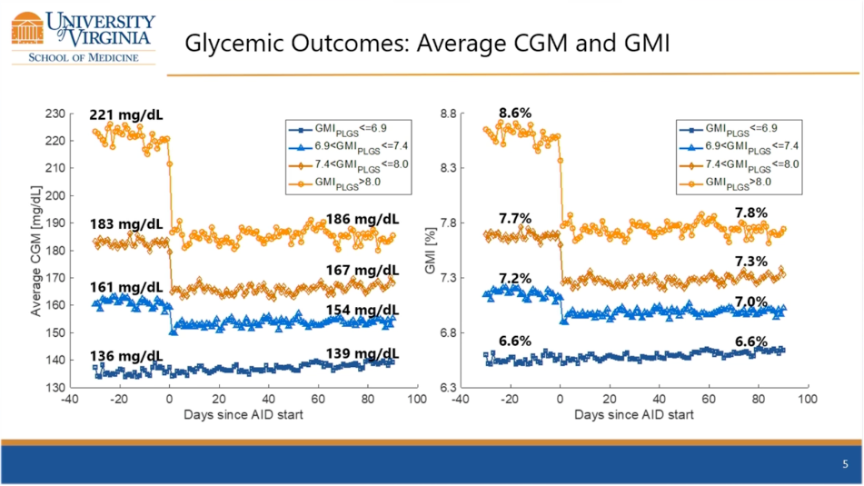
- As expected, there was a better outcome in those previously well regulated on the one hand, and more improvement in those previously worse regulated on the other.
- The TBR did not seem to differ significantly.
So again, these results are similar to the effect of Tandem Control in Type 1 diabetes.
What's next?

- Sometime in the 2nd half of 2023, the Mobi pump will be launched in America, a semi-patch pump 50% smaller than the t:slim X2 pump.
- Through a "Tandem Choice Programme", people using the t:slim X2 will be able to switch to the Mobi at no extra cost, even if their t:slim X2 pump is still in warranty.
- The expected update of Tandem Control for integration of the Dexcom G7 (2nd half 2023) and Libre3 (2023/2024) will also be offered to users at no additional cost.
- An update of the t:connect platform to the newer Tandem Source (in America, that is) is also expected this summer.
- And Tandem is also working on a fully closed-loop system, after all...

3. Omnipod 5

Slow rollout of Omnipod 5 in Europe
According to Insulet's latest quarterly update, there are now 100 000 people using the Omnipod 5 in America.
The Omnipod 5 has had a CE label since 1-2023, but the rollout in Europe is very slow.
- UK will be allowed to start first in mid-2023, and only in late 2023 will Germany be allowed to start.
- The rest of Europe will have to wait until 2024.
The slow commercialisation is said to be due to the need for data privacy approvals, which vary from country to country.
- Indeed, Omnipod 5 works with real-time uploads to Glooko via a built-in SIM card in their PDM.
- Also, the Omnipod 5 app would not yet be available in Europe in a first phase.
Only people at lowest target value achieve average TIR of 71%

At the ATTD2023, real-world data were shown from the first n=31 691 Omnipod 5 users in America.
- No average overall TIR was shown, only a breakdown of the TIR when using the different target values. Here it is notable that only a TIR of around 70% is achieved when using the lowest target value.
- At a target value of 110 mg/dl or 6.1 mmol/l, people achieve a TIR of 71%,
- At a target value of 120 mg/dl or 6.7 mmol/l, a TIR of 63% is achieved,
- and at a target value of 130-150 mg/dl or 7.2-8.3 mmol/l, the average TIR is only 55%.
- However, the low % TBR is striking: only 1.2% even at the lowest target value.
Adolescents do not achieve mean TIR >70% despite Omnipod 5 with lowest target value

Within the group using the lowest target value of 110 mg/dl o f 6.1 mmol/l, there was some variation based on age.
- The youngest children and adults >65 years achieved the best results with a TIR of around 75%.
- Adolescents had the most difficulty in achieving good glycaemic control, with a TIR of around 65%.
Better results if you bolus ≥ 4x/d

From the real-world data, we also learn that those who bolus a lot (≥4x/d) achieve better results.
This is consistent with associations noted in past real-world users of Tandem Control IQ and MiniMed 780G.
In the first few months, the carbohydrate ratio will probably need to be "strenghtened" by 10-20%

A data analysis of the pivotal study showed that after 3 months of using the Omnipod 5, carbohydrate ratio was strenghtened by 11à20%, indicating that healthcare providers should be prepared to strengthen (lower) carbohydrate ratio if necessary to prevent postprandial hyperglycaemia (click here for poster and accompanying audio).
- Also interesting was that if you use the 450 rule, you will probably underestimate the carbohydrate ratio by 13-22% for people aged 10 years and above, and by 40-49% for children <10 years.
- Looking at the average carbohydrate ratio with Omnipod 5, it also seems to be slightly lower than with the Minimed 780G cfr average carbohydrate ratio in adults was 8.3 g/E.
"Easy to teach and easy to learn"

Of course, all this new technology raises questions about how much time and energy it will take to explain all this to people who will actually have to use it.
One of the features of patch pumping, though, is that learning it is easier.
This has now been demonstrated in this study with 48 diabetes educators from UK and 27 educators from Germany.
- The time taken to start up the Omnipod DASH (n=105) was compared with the time taken to start up a tubed pump (n=164)
- For the Omnipod DASH, this would have been only 107 minutes, 15 minutes less than for a tubed pump.
- In doing so, no difference was noted between a virtual explanation or an explanation face-to-face.
Future research Omnipod 5

Insulet said it was working on the following priorities:
- Omnipod 5 in people with type 2 diabetes:
- the first study with 24 adults showed good results (Davis et al. Diabetes Care 2023),
- and a "pivotal" study with 350 people with type 2 diabetes will start in America within weeks (SECURE-T2D).
- Omnipod 5 in hospital: the first study in 16 people with type 1 and type 2 diabetes has been completed (AIDING Feasability Trial)
- Omnipod 5 immediately after diagnosis of type 1 diabetes in children: this French study was initiated in 112 children (AP-AT-DIAGNOSIS)
What's next?

Insulet reiterated their plans to market a basic Basal-Only Pod by 2024 for adults with type 2 diabetes.
- It is not controlled by a controller and so no settings can be entered.
- It only contains a fixed dose of basal insulin.

Also named, but with no timeline:
- the integration of Dexcom G7 and Libre sensor into Omnipod 5
- and an Omnipod 5 app for iPhone.
4. Diabeloop

Real-world data from 6 658 users
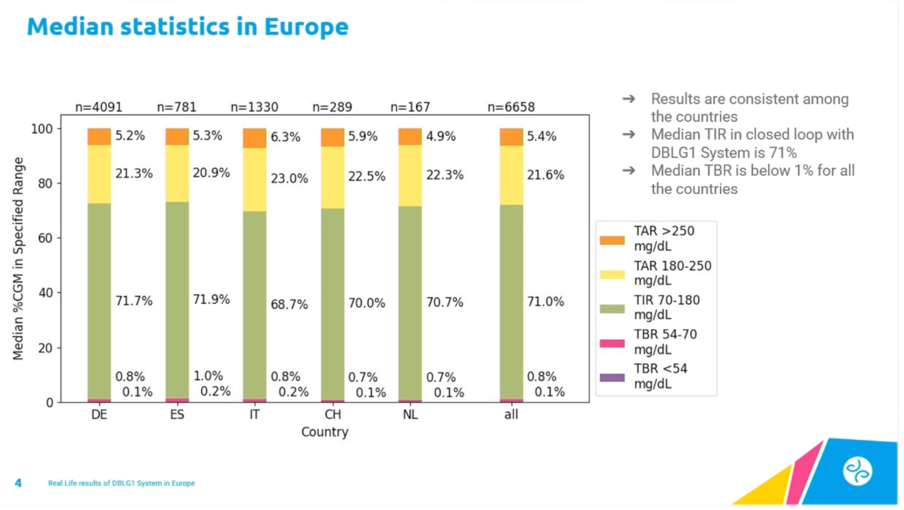
At the ATTD2023, real-world data were shown from 6 658 users of DBLG1 in Germany, Spain, Italy, Switzerland and the Netherlands.
- The mean overall TIR was 71% and TBR only 0.8%.
- These glycaemia results were relatively stable across the 5 countries.
Lessons from real-world data: adjust your settings regularly

When reviewing real-world data from Germany, a clear correlation was noticed between adjusting your target value and your glycaemic control.
From this, it was concluded that it does make sense to adjust your target value from time to time.
Full closed-loop system under development
Diabeloop announced that they have started a study in 50 adolescents with type 1 diabetes with a completely closed-loop algorithm, thanks to their Unannounced Meal Management (UMM) module.
Initial results are said to be promising.
5. CamAPS FX

Real-world data from 1 805 users

Real-world data from 1805 users of CamAPS FX were shown at ATTD2023.
- The mean TIR was 73% and TBR 2.3%.
- The youngest children ≤6 years performed slightly less well with a TIR 67% and TBR 3.0%.
- The high time in auto mode (95%) indicates good system portability.
Strengthening carbohydrate ratio has less effect in CamAPS FX

Prof Dr Roman Hovorka went over the propositions from a recent very interesting opinion piece (Messer et al DTT 2023).
He agreed with most of the propositions, except for the need to intensify the carbohydrate ratio.
- In fact, CamAPS FX has a self-learning algorithm, based on trends overall, diurnal and post-meal to optimize the automated insuline delivery.
- If you use an overly strong / "low" carbohydrate ratio resulting in large meal boluses, this post-meal self-learning algorithm is suppressed to prevent hypoglycaemia.
- This can then lead to more erratic post-meal glycaemia.
Launch mylife Loop with Libre3 in UK, Netherlands and Switzerland in mid-2023

Mylife Loop is the CamAPS algorithm combined with the Ypsopump. (CamAPS with the Dana pump will not be commercialized outside of UK).
You can choose 2 sensors here:
- mylife Loop with Dexcom G6: this is already available in several European countries
- or mylife Loop with Libre3: this is already used without problems by 450 people with type 1 diabetes in Germany.
The additional option for the Libre3 will also become available in the UK, the Netherlands and Switzerland in mid-2023.
If you choose Libre3, you can avoid data loss during the warm-up period
Normally, during the warm-up period of your sensor, you have no data for your closed-loop system. Most systems then switch to manual mode for 1 to 2 hours.
With the Libre sensors, the warm-up period is only 1 hour compared to 2 hours compared to Dexcom G6 and Guardian 4, but even for that one hour, a solution is now proposed.
- It would not be a problem to already start the new Libre3 sensor while the previous Libre3 sensor is still running.
- That way, your new Libre3 sensor is fully warmed up by the time you let it be used by the mylife Loop app, and you don't have to interrupt your closed-loop every time you replace your sensor.
With the Dexcom and Guardian sensor, this is not possible because you need the transmitter from the old sensor, to start the new sensor.
New: CamAPS Companion app for carers
There is a new way to monitor people remotely, namely the CamAPS Companion app (cfr press release Ypsomed).
- This "mirroring" app allows parents to see all the information as on the mylife Loop app itself.
- In time, this app will replace the current real-time SMS alerts.
New: easier sharing of reports
For now, CamAPS FX reports can only be read with Diasend, the old version of Glooko.
The connection to Glooko is planned, but is not there at the moment.
However, there is now an easier way to send the PDF reports from the app directly to the healthcare provider (cf. video).
You can see what the reports look like in this fact sheet.
6. INREDA

INREDA has been developing a bihormonal closed-loop system with insulin and glucagon for >10 years.
Their AP5 is currently being evaluated
- in a randomised study with 240 adults with type 1 diabetes in the Netherlands for 12 months (DARE study)
- and in a crossover study with 20 adolescents (12-18 years) with type 1 diabetes in the Netherlands for 3 weeks
No word yet on interim results.
Presentation of the AP6

At the ATTD2023, the AP6 was shown for the first time.
It is slightly nicer in design, and also smaller and thinner than the AP5.
Its commercialisation is planned for 2025.

Combined sensor and infusion set

INREDA also indicated at the ATTD2023 that they will evolve from 4 to 2 contact points on the body, switching to a combined sensor and infusion set.
They will, however, stick to the need for 2 sensors and 2 infusion sets.
This is planned for 2028.
7. Project Liberty

Dexcom bought TypeZero, the algorithm behind Control IQ, in 2018 and has now developed its own "next-generation TypeZero" algorithm based on computer simulators for the first time.
At ATTD2023, this was officially presented as "Project Liberty".
No user interaction required/possible

The "Liberty" algorithm is a fully closed-loop algorithm for people with type 1 as well as type 2 diabetes who do not want to interact with the system.
- It is based on 1 parameter, namely the total daily dose of basal insulin/24, and adjusts the insulin based on the sensor data of the last 2 weeks.
- You can only turn the system on or off.
- You cannot enter meals, set temporary target values (e.g. for sport or sleep) or set a higher aggressivity.
Combination with YpsoPump instead of Tandem t:slim X2

The closed-loop system consists of three parts:
- a Dexcom G6 sensor,
- the Liberty algorithm on a mobile phone,
- and a YpsoPump - fairly surprising as TypeZero previously partnered with Tandem Pumps
Moderate results for now

It has already been tested in 15 people for 84 days:
- The TIR increased from 35% to 55%: a nice 20% increase, but still well below the 70% usually assumed to be adequate glycaemic control in people with diabetes.
- However, Liberty was developed primarily to avoid severe hyperglycaemia (>250 mg/dl or >13.8 mmol/l) and severe hypoglycaemia (<54 mg/dl or <3.0 mmol/l), and it did manage to do so reasonably well.
Further research

Dexcom makes the case that they have been able to develop this algorithm very quickly thanks to simulators,
and that with the help of pattern recognition and artificial intelligence, they will be able to further improve the algorithm.
Further research on 40 people in New Zealand is planned.
These various updates on closed-loop systems show that more closed-loop systems are gradually appearing on the market. Hopefully, this competition will bring down the price, as currently, far from everyone with type 1 diabetes will be reimbursed for closed-loop systems, even though this is recommended.
The ATTD congress is crucial for creating awareness on this issue. Important and influential professors spoke at length about the importance of closed-loop systems and the need to start them early after diagnosis of type 1 diabetes to prevent complications.
Meanwhile, all companies are working to take steps towards fully closed-loop systems, which eliminate the need for indicating meals. A key question that was often asked was: what Time in Range (TIR) can people with diabetes and caregivers accept if there is no longer a need to bolus? This is because a fully closed-loop system will always sacrifice some glycaemic control compared to entering the grams of carbohydrates. There is currently no consensus on this open question.
Surveys also show that people still want to be able to notify the system when they 'sin'. They also want to be able to specify the size of their meal (e.g. normal portion, small or large portion). The companies hereby know what to do next.
If you are curious about what they can achieve, be sure to put ATTD2024 in your diary: it will take place from 6-9 March 2024 in Florence.
Kind regards,
![]()