Diabetes Devices: When the Skin Says No
Jul 06, 2026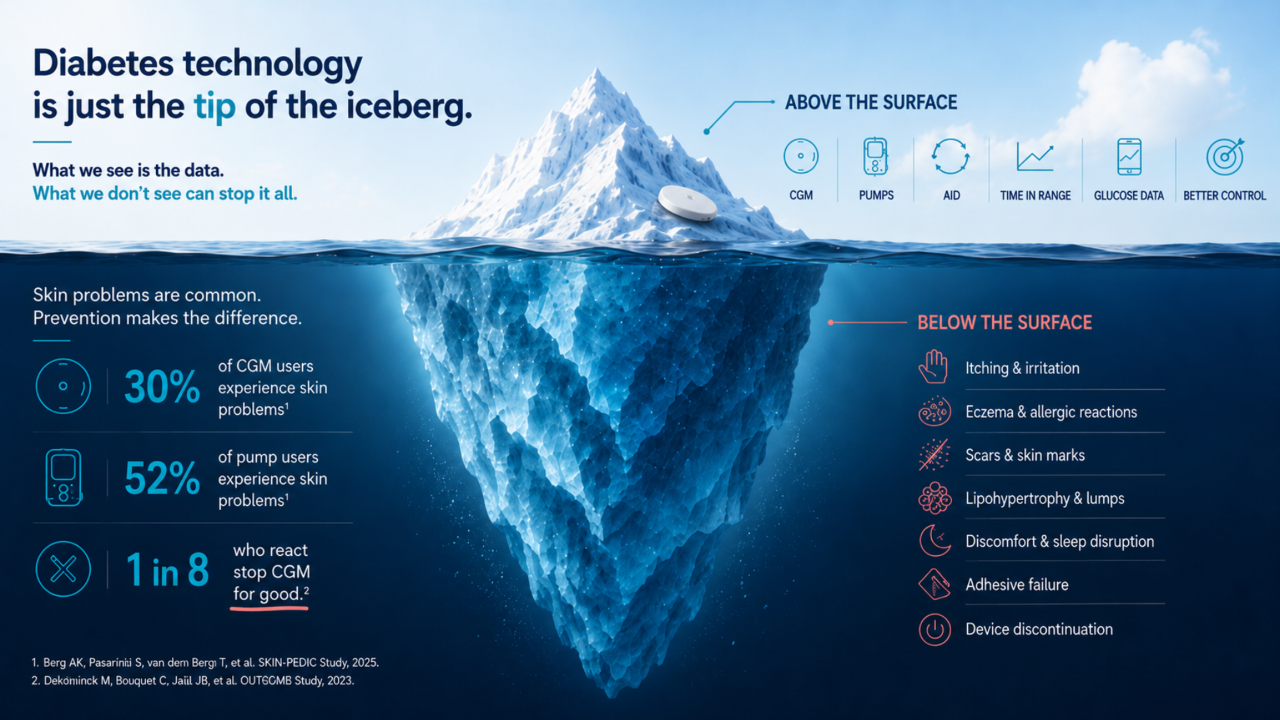
Prevention, Recognition and Treatment of CGM and Insulin Pump Skin Problems - The Forgotten Complication of Diabetes Technology
We talk a lot about Time in Range, algorithms, and automation.
We compare sensors, pumps, and hybrid closed-loop systems.
Yet for some people, the greatest challenge is much simpler:
Finding a patch of healthy skin that can tolerate another sensor or infusion set.
The most advanced diabetes technology in the world is useless if the skin can no longer tolerate it.
As diabetes devices become increasingly integrated into daily life, skin health is emerging as an important — and often underestimated — part of successful device use.
Skin reactions do not only affect comfort. They can disturb sleep, reduce confidence in diabetes technology, and ultimately lead to device discontinuation.
The multinational SKIN-PEDIC study found that:
- 30% of CGM users experienced skin problems
- 52% of insulin pump users experienced skin problems
And beyond these visible reactions, the single most common complaint is something simpler: itching.
Across studies, itching is reported by anywhere from 23% to 77% of people wearing a sensor or pump.
It is easy to dismiss as trivial. It isn't. Itching has been linked to reduced concentration at school, disturbed sleep, and devices loosening as people scratch — which in turn damages the skin barrier and makes the next reaction more likely.
In adults, the CUTADIAB study reported skin reactions in 28% of CGM users and 29% of insulin pump users.
Most of these reactions pointed to irritation rather than true allergy, and the large majority of people kept using their device.
But not everyone could. Among those who reacted, 12% eventually stopped CGM for good — around 3% of all CGM users in the study.
A small fraction. Not zero.
And every one of them represents a preventable loss of therapy — not because they disliked the technology, but because their skin could no longer tolerate it.
Not all skin reactions are the same. Identifying the problem is the first step toward finding the right solution.
| Problem | Typical Appearance | Common Symptoms | Most Likely Cause | How Common? |
| Irritant eczema | Red patch under adhesive | Burning, dryness, mild itching | Friction, sweat, adhesive trauma | Very common |
| Allergic eczema | Bright red rash, sometimes blisters | Intense itching | Allergy to adhesive ingredients | Less common |
| Scarring | Dark or light marks, thickened skin | Usually none | Repeated insertions | Very common in long-term users |
| Lipohypertrophy | Lump beneath the skin | Usually painless | Repeated insulin delivery in same area | Common in pump users |
| Infection | Red, swollen, painful area | Pain, warmth, pus | Bacterial infection | Uncommon |
What Skin Problems Can Occur?
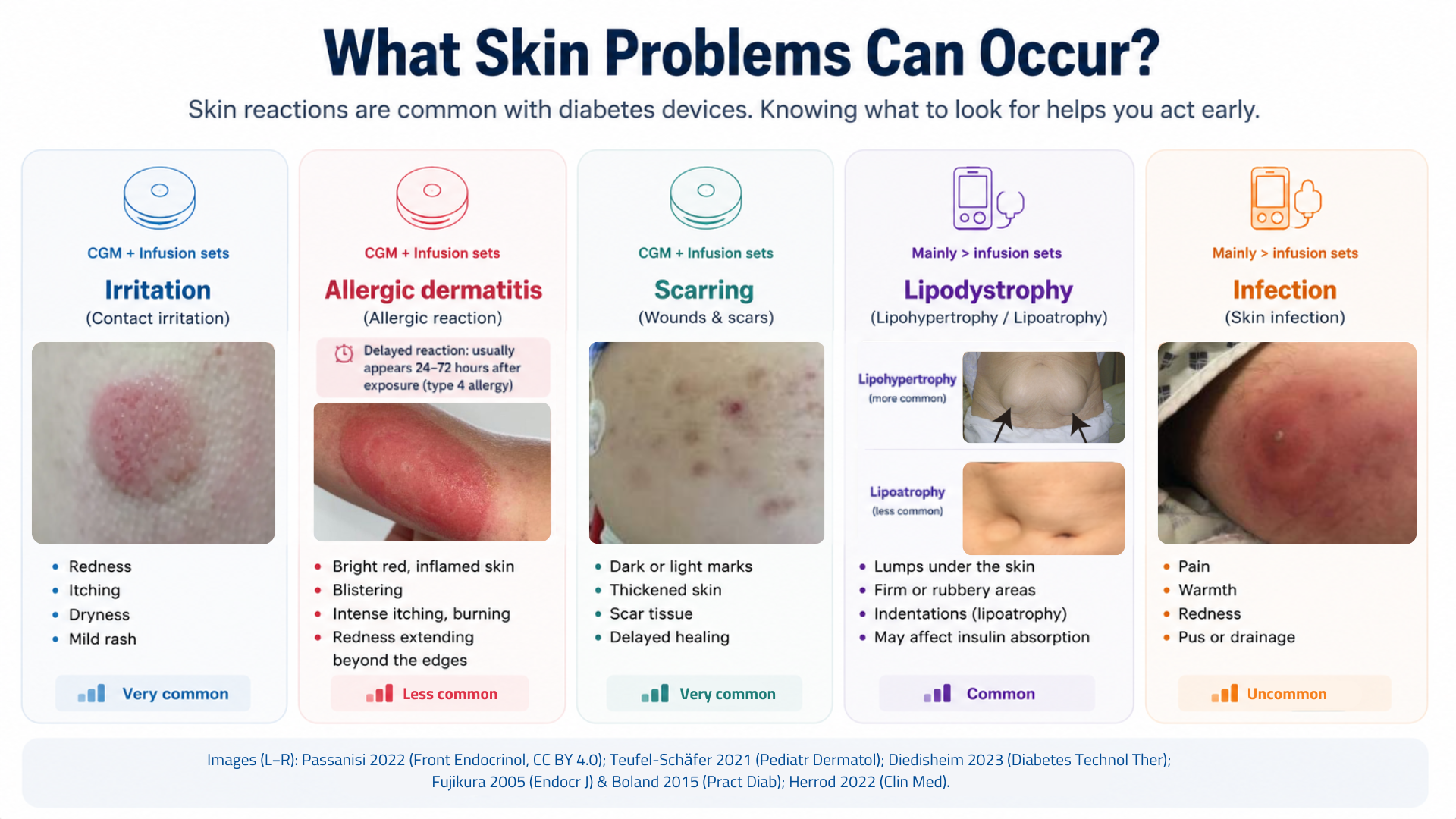
Most device-related skin problems fall into four broad categories:
- Skin irritation and eczema
- Scarring and tissue changes
- Lipodystrophy (changes in fatty tissue beneath the skin)
- Infection
Understanding the difference is important because treatment depends on the underlying cause.
Skin Irritation and Eczema
The most common skin problems occur beneath the adhesive patch and are usually referred to as contact dermatitis or eczema.
Typical symptoms include:
- Redness
- Itching
- Burning
- Dryness
- Swelling
- Blistering
Although these reactions may look similar, two different mechanisms can be responsible.
*Irritant Eczema (Irritant Contact Dermatitis)
Irritant eczema is the most common type of skin reaction.
It develops when the skin barrier becomes damaged over time through:
- Repeated adhesive removal
- Friction
- Sweat and moisture
- Heat
- Prolonged wear
Anyone can develop irritant eczema if the skin is exposed long enough.
The reaction is caused by skin damage rather than allergy.
*Allergic Eczema (Allergic Contact Dermatitis)
Allergic eczema is less common but often more severe.
Rather than being caused by skin damage, it results from an immune reaction against chemicals present in the adhesive.
Clues suggesting an allergic reaction include:
- Intense itching
- Blistering
- Bright red inflammation
- Rash extending beyond the adhesive border
A key feature of allergic eczema is that it is often delayed.
Symptoms typically appear 24–72 hours after exposure and may develop only after weeks, months, or even years of successful device use.
Once allergy develops, future exposures often trigger faster and more severe reactions.
When allergy is the culprit, the trigger is almost always a chemical in the adhesive, the device housing, or the glue that holds the device together — not the plastic you can see.
The best-known offender is isobornyl acrylate (IBOA), an adhesive-curing chemical that sensitised hundreds of documented patients after appearing in one widely used sensor. But it is far from the only one. Others repeatedly implicated include:
- Other acrylates (for example 2-phenoxyethyl acrylate, 1,6-hexanediol diacrylate)
- N,N-dimethylacrylamide (DMAA)
- Colophonium (rosin) and its derivatives — notably, this one also turns up in some adhesive-remover and barrier products, so the "fix" can occasionally become the problem
- Diisocyanates used in certain infusion sets
- Phenolic antioxidants and photoinitiators (such as BHT and di-tert-butylphenol)
*How pervasive are these chemicals?
A 2025 chemical analysis of 27 diabetes devices found that every single product tested contained at least one chemical previously reported to cause allergic contact dermatitis — acrylates in about half, colophonium derivatives in a third, and phenolic compounds in all of them.
An important, often-missed point: the allergen is sometimes hidden in the glue that fixes the needle into the plastic housing, not in the peel-off adhesive at all. When that is the case, barrier films and overpatches placed under the adhesive will not help — the person may need a spacer approach or a different device entirely.
Manufacturers still do not consistently disclose full adhesive composition, which makes both prediction and patch testing harder than it should be.
Scarring and Tissue Changes
Repeated insertion and removal of sensors and infusion sets can gradually lead to:
- Small scars
- Darker skin marks
- Lighter skin marks
- Thickened skin
- Delayed healing
These changes often develop slowly and may be even more common than eczema among long-term device users.
Although usually cosmetic, scar tissue can make future insertions more difficult and reduce the number of suitable sites available.
Lipodystrophy: Changes Beneath the Skin
For people using insulin pumps, repeatedly delivering insulin into the same area can gradually change the fatty tissue beneath the skin.
The most common consequence is lipohypertrophy: a build-up of thickened fatty tissue that feels like a lump beneath the skin.
Less commonly, lipoatrophy may occur, causing visible dents or loss of fatty tissue.
Lipohypertrophy is often painless and can develop gradually, making it easy to miss.
*Typical signs include:
- Firm or rubbery lumps beneath the skin
- Areas that feel thicker than surrounding tissue
- Repeated use of the same infusion sites
- Unexplained glucose variability
- Increased insulin requirements
*Why does this matter?
Because insulin absorbed from lipohypertrophic tissue becomes less predictable. As a result, glucose levels may fluctuate more, correction doses may seem less effective, and insulin requirements may increase over time.
For this reason, healthcare professionals should routinely inspect and palpate infusion sites during diabetes visits.
*Can Ultrasound Detect Problems Earlier?
Not always.
Many areas of lipohypertrophy can be detected by careful inspection and palpation, but some tissue changes develop before a lump becomes visible or palpable.
High-frequency ultrasound can identify these early changes and is considerably more sensitive than physical examination alone. Studies suggest that a substantial proportion of lipohypertrophy lesions may be missed during routine clinical examination.
For this reason, the 2025 FITTER Forward recommendations recognize ultrasound as a sensitive and objective method for detecting lipohypertrophy and recommend its use when available.
However, ultrasound is not routinely available in most diabetes clinics. For now, regular site rotation combined with careful inspection and palpation remains the cornerstone of prevention and detection.
*The Good News
Lipohypertrophy is largely preventable.
Consistent site rotation remains one of the most effective strategies for preserving healthy tissue and maintaining reliable insulin absorption over the long term.
Healthcare professionals should routinely inspect and palpate infusion and injection sites, as lipohypertrophy may be present even when site rotation is reported.
Infection
Fortunately, infections remain relatively uncommon. However, they should be recognized promptly.
Warning signs include:
- Increasing redness
- Warmth
- Pain
- Swelling
- Drainage of pus
Unlike eczema, infections are often painful rather than itchy.
If these symptoms occur, medical assessment is recommended.
People with diabetes who have impaired wound healing or who are immunocompromised should be particularly attentive to signs of infection.
Who Is Most at Risk?
Some people appear more susceptible to device-related skin problems than others.
Known risk factors include:
- Childhood and adolescence
- A history of contact dermatitis
- Atopic dermatitis (eczema)
- Sensitive or easily irritated skin
- Long-term continuous use of diabetes devices
Among these factors, atopic dermatitis appears particularly important, substantially increasing the risk of skin reactions in some studies.
Two simple clues may help identify people with atopic dermatitis:
- Wool worn directly on the skin causes discomfort or itching.
- The palms contain an unusually large number of fine skin creases ("hyperlinear palms").
These observations highlight an important point:
Skin reactions depend not only on the device itself but also on the characteristics of the person wearing it.
Can Different Devices Cause Different Reactions?
Yes.
Although skin reactions can occur with any CGM or insulin pump, adhesives differ between manufacturers.
Potential contributors include:
- Different adhesive formulations
- Wear duration
- Heat and moisture retention
- Occlusion of the skin
- Individual allergies to specific ingredients
Some people react severely to one device but tolerate another without difficulty.
Unfortunately, manufacturers do not always disclose all adhesive ingredients, making predictions difficult.
For some individuals, switching devices may ultimately prove more effective than adding barrier products.
Importantly, tolerating one CGM or pump does not guarantee tolerance of another. Likewise, reacting to one device does not mean that all diabetes devices will cause problems.
Prevention: The Skin Care Checklist
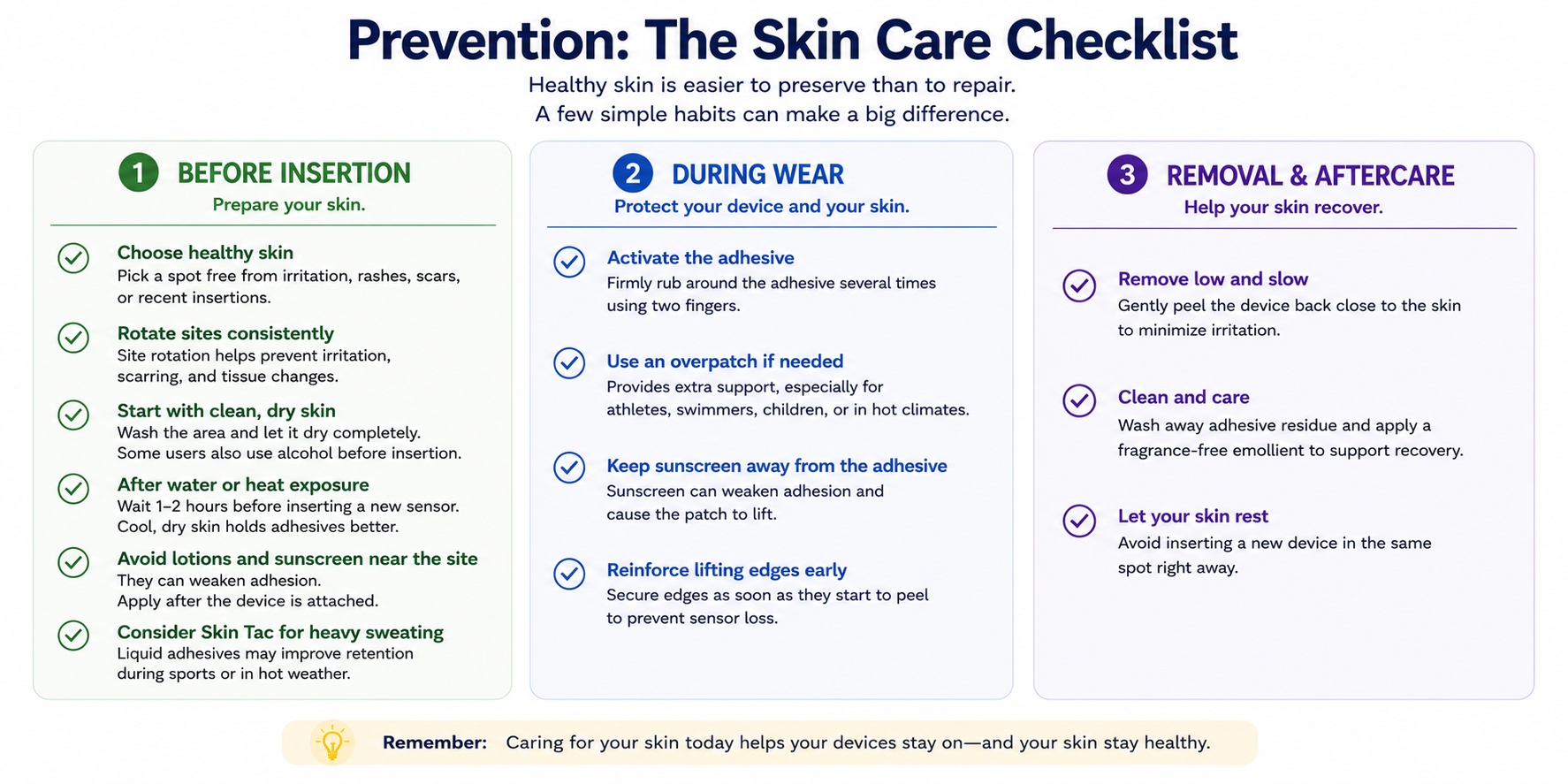
Healthy skin is easier to preserve than to repair.
Most skin reactions are easier to prevent than to treat.
Fortunately, a few simple habits can make a significant difference.
1. Before Insertion
Choose Healthy Skin
Select an area that is:
- Free from irritation
- Free from rashes
- Free from scars
- Free from recent insertions
Rotate Sites Consistently
Site rotation remains one of the most effective ways to prevent long-term skin complications.
Think of rotation as preventive maintenance for your skin.
Start With Clean, Dry Skin
Wash the area and remove:
- Oils
- Sweat
- Dirt
- Residual adhesive
Allow the skin to dry completely before insertion.
Use Alcohol Wipes If Needed
An alcohol wipe may help remove oils and improve adhesion. Allow the skin to dry completely before insertion.
Reduce Excessive Sweating
If you tend to sweat heavily, applying an unscented antiperspirant to the skin around the intended insertion site 10–15 minutes before insertion may help improve adhesion.
Avoid applying it directly where the sensor filament or infusion cannula will enter the skin. Allow it to dry completely before applying the device.
Wait After Water Exposure
Avoid applying a new device immediately after:
- Showering
- Swimming
- Bathing
- Sauna use
Waiting 1–2 hours allows the skin to return to its normal condition.
Trim Hair If Needed
Hair can interfere with adhesion and make removal more uncomfortable.
Trimming is often preferable to shaving immediately before insertion.
Avoid Lotions and Sunscreen Near the Site
Moisturizers, body oils, insect repellents, and sunscreen may reduce adhesion.
Apply these products after the device is secured and avoid direct contact with the adhesive.
Consider Additional Adhesive Support
For people who frequently lose sensors during exercise or hot weather, products such as Skin Tac may improve retention.
The goal is not maximum stickiness.
The goal is reliable adhesion with minimal skin trauma.
2. During Wear
Activate the Adhesive
Most adhesives are pressure-sensitive.
Firmly rubbing around the adhesive after insertion may significantly improve adhesion.
Use an Overpatch If Needed
Overpatches may be particularly useful for:
- Athletes
- Swimmers
- Children
- Heavy sweaters
- People living in hot climates
Keep Sunscreen Away From the Adhesive
Sunscreen may weaken adhesion and promote edge lifting.
Reinforce Lifting Edges Early
Small areas of peeling are easier to fix than complete device failure.
3. After Removal
This may be the most overlooked step of all.
Treat the skin between devices.
Remove Low and Slow
Peel adhesives back gently and close to the skin surface.
Slow removal reduces skin trauma.
For stubborn adhesives, adhesive remover wipes or sprays may reduce skin trauma during removal.
Clean and Care for the Skin
After removal:
- Remove adhesive residue
- Inspect the skin
- Apply a fragrance-free emollient if the skin is intact
Allow Recovery Time
Avoid placing the next sensor or infusion set in exactly the same location.
Healthy skin today increases the chance of successful device wear tomorrow.
A Stepwise Approach to Skin Reactions
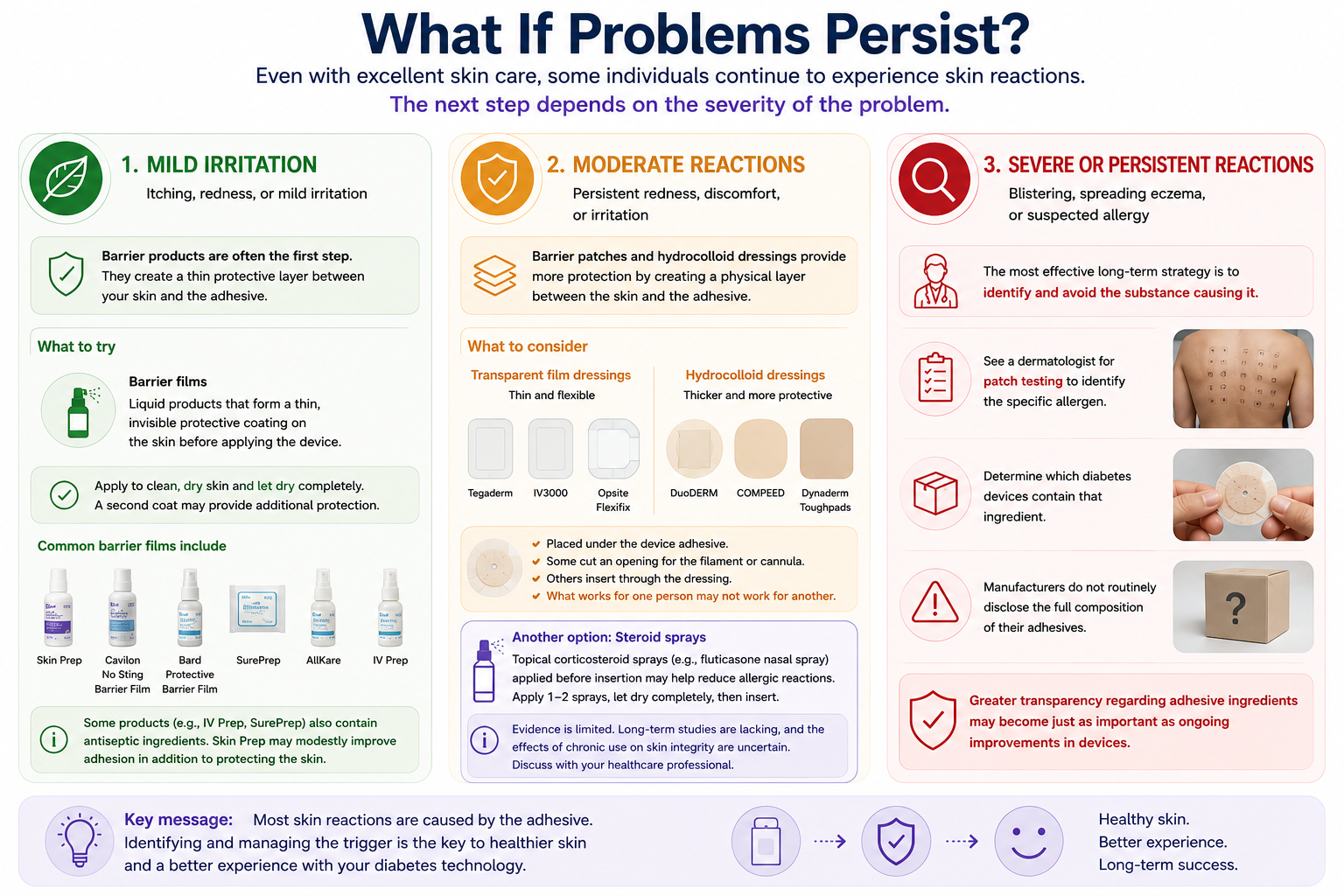
Even with excellent skin care, some people continue to experience skin reactions.
A stepwise approach often works best.
Step 1: Mild Redness or Itching
Try:
- Optimizing skin care
- Improving site rotation
- Using a barrier film
Common barrier films include:
- Skin Prep
- Cavilon No Sting Barrier Film
- Bard Protective Barrier Film
- SurePrep
- AllKare
- IV Prep
Barrier films create a thin protective layer between the skin and the adhesive while preserving adhesion.
For many people, this simple intervention is sufficient.
Step 2: Persistent Irritation
If symptoms continue despite barrier films, additional protection may help.
Transparent Film Dressings
Examples include:
- Tegaderm
- IV3000
- Opsite Flexifix
These products are thin and flexible.
Hydrocolloid Dressings
Examples include:
- DuoDERM
- COMPEED
- Dynaderm
- Toughpads
These are generally thicker and provide greater protection.
Some people cut a small opening for the sensor filament or infusion cannula.
Others insert directly through the dressing.
Skin reactions are highly individual.
What works perfectly for one person may not work at all for another.
*What About Steroid Sprays?
Another strategy attracting increasing interest is the use of topical corticosteroid sprays such as fluticasone nasal spray before insertion.
The usual approach involves:
- Spraying the intended insertion site.
- Allowing it to dry completely.
- Applying the device.
Early reports are encouraging, but evidence remains limited.
Long-term safety data are lacking.
For selected individuals with recurrent hypersensitivity reactions, this strategy may be worth discussing with a healthcare professional.
Step 3: Severe or Persistent Reactions
If significant itching, eczema, blistering, or recurrent reactions continue despite preventive measures, the next step is often identifying the trigger.
This typically involves:
Dermatology Assessment
A dermatologist can evaluate whether allergic contact dermatitis is present.
Patch Testing
Patch testing can identify the specific allergen responsible for the reaction.
Once the allergen is identified, avoiding products containing that ingredient becomes possible.
Unfortunately, this process is often complicated by incomplete disclosure of adhesive ingredients by manufacturers.
As diabetes devices become increasingly sophisticated, greater transparency regarding adhesive composition may become just as important as improvements in sensor accuracy and automated insulin delivery.
When Should You Seek Medical Advice?
Contact your healthcare team if:
- The rash spreads beyond the adhesive borders.
- Blisters develop.
- The reaction worsens with each new device.
- The skin becomes painful rather than itchy.
- Pus or drainage appears.
- You are considering stopping CGM or pump therapy because of skin problems.
Practical Tips for Healthcare Professionals
When evaluating device-related skin reactions:
Ask
- When did symptoms begin?
- Is itching or pain the dominant symptom?
- Does the rash extend beyond the adhesive?
- Has the patient recently switched devices?
- Is there a personal history of eczema or allergies?
Examine
Look for:
- Infection
- Lipohypertrophy
- Scarring
- Distribution patterns
Consider Referral
Referral to dermatology should be considered when:
- Reactions are severe
- Blistering occurs
- Patch testing may influence future device choice
- Device discontinuation is being considered
Distinguishing irritant from allergic contact dermatitis is often the most important clinical decision, as management strategies differ substantially.
Frequently Asked Questions
Can I become allergic after years of successful device use?
Yes. Allergic contact dermatitis may develop months or even years after first exposure.
Can I continue wearing my sensor if I have a mild rash?
Many people can continue using their device while implementing preventive measures, but worsening symptoms, blistering, or signs of infection warrant medical review.
Can I insert a sensor through a hydrocolloid dressing?
Many users do, although manufacturer recommendations vary.
Which barrier film works best?
There is no single best product. Individual responses vary considerably.
Do skin reactions affect sensor accuracy?
Most mild reactions do not affect sensor performance directly, but severe reactions may shorten wear time by compromising adhesion.
Which CGM causes the fewest skin reactions?
Current evidence does not support one device as universally superior. Individual tolerance varies substantially.
Key Takeaways
✓ Skin problems are common among people using CGMs and insulin pumps.
✓ Prevention is easier than treatment.
✓ Consistent site rotation is essential.
✓ Healthy skin should be considered part of diabetes management.
✓ There is no single solution that works for everyone.
✓ Persistent reactions warrant professional evaluation.
The Bottom Line
The future of diabetes technology is becoming increasingly automated, intelligent, and personalized.
Yet every sensor, every infusion set, and every insulin pump still depends on one thing:
Healthy skin.
Protecting the skin is not a cosmetic issue. It is an essential part of successful diabetes technology use.
Because even the most advanced device cannot help if the skin beneath it can no longer say yes.
=> Diabetes technology continues to evolve rapidly. If you would like to stay informed about new developments, practical troubleshooting strategies, and evidence-based educational resources, you can subscribe to the Diabetotech blog.
References
- Berg AK, Passanisi S, von dem Berge T, et al. SKIN-PEDIC: A worldwide assessment of skin problems in children and adolescents using diabetes devices. Horm Res Paediatr. 2025.
- Diedisheim M, Pecquet C, Julla JB, et al. Prevalence and description of the skin reactions associated with adhesives in diabetes technology devices in an adult population: Results of the CUTADIAB study. Diabetes Technol Ther. 2023;25(4):279–286.
- Messer LH, Berget C, Beatson C, Polsky S, Forlenza GP. Preserving skin integrity with chronic device use in diabetes. Diabetes Technol Ther. 2018;20(Suppl 2):S254–S264.
- Passanisi S, Salzano G, Galletta F, et al. Technologies for type 1 diabetes and contact dermatitis: therapeutic tools and clinical outcomes in a cohort of pediatric patients. Front Endocrinol. 2022.
- de Groot A, van Oers EM, Ipenburg NA, Rustemeyer T. Allergic contact dermatitis caused by glucose sensors and insulin pumps: a full review. Contact Dermatitis. 2025.
- van Oers EM, et al. Results of GC–MS Analyses of 40 Extracts of Diabetes Devices. Contact Dermatitis. 2026
- Teufel-Schäfer U, Huhn C, Müller S, Müller C, Grünert SC. Severe allergic contact dermatitis to two different continuous glucose monitoring devices in a patient with glycogen storage disease type 9b. Pediatr Dermatol. 2021;38(5):1302–1304. doi:10.1111/pde.14767.
- Fujikura J, Fujimoto M, Yasue S, Noguchi M, Masuzaki H, Hosoda K, et al. Insulin-induced lipohypertrophy: Report of a case with histopathology. Endocr J. 2005;52(5):623-628.
- Boland X, Chenoweth H, Sulkin T, Browne D. Progressive and disabling lipoatrophy associated with insulin aspart via continuous subcutaneous insulin infusion. Pract Diab. 2015;32:336-337a. doi:10.1002/pdi.1985.
- Herrod SS, Liversedge G, Vaidya B, Walker N. Continuous glucose monitoring for diabetes: Potential pitfalls for the general physician. Clin Med (Lond). 2022;22(5):482-484. doi:10.7861/CM-2022-0199.R1.
-
Kapeluto JE, Paty BW, Chang SD, Meneilly GS. Ultrasound detection of insulin-induced lipohypertrophy in Type 1 and Type 2 diabetes. Diabet Med. 2018;35(10):1383–1390.
-
Yang H, Zhang L, Dong Q, et al. The distinct ultrasound characteristics and prognostic features of insulin-induced lipohypertrophy: a systematic review. Diabetes Metab Syndr Obes. 2025;18:941–954.
-
Sun ZH, Yu CH, Wang X. Exploring the diagnostic value of high-frequency ultrasound technology for subcutaneous lipohypertrophy in diabetes patients receiving insulin injections. Diabetes Metab Syndr Obes. 2024;17:1359–1366.
-
Klonoff D, Berard L, Franco D en al. Advancing insulin injection technique and education with FITTER Forward expert recommendations. Mayo Clin Proc. 2025.