Update ISPAD 2022
Oct 29, 2022
The pediatric endocrinologists have their own organization which is the International Society for Pediatric and Adolescent Diabetes or ISPAD.
Their annual convention took place this month in Abu Dhabi, and as expected we heard some interesting updates on diabetes technology:
- MiniMed 780G: fixed boluses work (almost) as well as carb counting
- Tandem Control IQ and Minimed 780G also work well with very young children (2-6 years)
- Open-source closed-loop systems are "still in the game"
Get Access To Updated Diabetes Technology Courses
Continue reading below to learn more details!
1. MiniMed 780G: fixed boluses work (almost) as well as carb counting

Carbohydrate counting is not easy, and is seen as one of the biggest difficulties when using closed-loop systems.
2/3 of adults would underestimate their carbohydrate portion by >20%.
Several closed-loop systems therefore move away from carb counting and use simple meal announcements:
- With CamAPS FX it is still recommended to count your carbohydrates, but you can also choose a preset number of carbohydrates (4 servings configured).
- With Diabeloop you no longer have to count carbohydrates, but you have to set the average number of carbohydrates per type of meal (breakfast, lunch and dinner) at the start. If you want to eat, you only indicate which meal portion you are going to eat (small, medium or large). You can also opt for a snack, which is set at 20 grams of carbohydrates.
- With the iLet insulin-only you no longer have to count carbohydrates, and you don't even have to enter a typical carbohydrate portion per meal at the start. If you want to eat, you can only enter the type of meal you are going to eat (breakfast, lunch or dinner) and its size (normal, more than usual, less than usual or much less than usual).
- The Omnipod 5 also has been tested with meal announcements instead of carbohydrate in people with type 2 diabetes.

Also with the MiniMed 780G it was now investigated whether a simple meal announcement would provide as good glycemic control as carbohydrate counting, and that appears to be the case!
34 adolescents (12-18 years, baseline HbA1c 7.9%-8.0%) were randomized to carbohydrate counting or a simple meal announcement such as "regular meal", "large meal" or a "snack".
The total daily dose of carbohydrates was calculated on the basis of a 7-day logbook, and the carbohydrates per type of meal were calculated on this basis:
- For a regular meal, 1/3 of 60% of the total daily dose of carbohydrates was assumed.
- For a large meal, they took 150% of a regular meal
- And for a snack 50% of a regular meal.
After 3 months, the glycemic control was found to be largely similar between the 2 groups:
- In the group using the MiniMed 780G with standard carbohydrate counting, the TIR increased from 49% to 80% (mean glycemia 145 mg/dl)
- In the group that used fixed boluses, the TIR increased from 48% to 74% (mean glycemia 147 mg/dl)
In addition, 88% of the group who worked with the fixed boluses chose to continue with this simpler method of meal bolusing.
This shows that the elimination of carbohydrate counting was much appreciated.
By working with a fixed number of grams of carbohydrates per meal, the calculation of the meal bolus will certainly not always have been correct.
However, it appears that this lower precision in carbohydrate counting can be accommodated by the algorithm of the MiniMed 780G.
It's clear that more and more companies are working to simplify their closed-loop systems so that they can be used by even more patients with diabetes.
While in the past we only started closed-loop systems when patients had proven that they can count carbohydrates, this may be less necessary than we thought (with the MiniMed 780G).
People who are not able to count carbohydrates or who really don't like this, may therefore also be able to work with fixed boluses, and let the system take care of the rest.
It seems safer to round the fixed carbohydrate portions down if you look at the calculation that was used here:
"number of carbohydrates per meal = 1/3 of 60% of the average number of grams of carbohydrate intake per day (calculated based on 7 days log)"
2. Tandem Control IQ and Minimed 780G also work well with very young children (2-6 years)

Currently, 2 out of 5 available commercial AID systems have been approved for very young children:
- CamAPS FX (and therefore also mylife Loop)
- was the first with a CE label for children from 1 year. This system does use the Dexcom G6, which is actually only approved from 2 years.
- The minimum total daily dose of insulin is 5 U.
- Omnipod 5
- has had an FDA label since this summer and even a CE label from the age of 2.
- The minimum total daily dose of insulin is 6 U.
- Tandem Control IQ
- is approved from 6 years, but ISPAD 2022 showed results of their study in children 2-5 years cfr infra.
- The minimum total daily dose of insulin is 10 U.
- Minimed 780G
- is approved from 7 years, but at ISPAD 2022 results were shown from their study in children 2-5 years cfr infra.
- The minimum total daily dose of insulin is 8 U.
- The MiniMed 670G and 770G (the predecessors of the MiniMed 780G) are already approved from 2 years.
- Diabeloop's
#1 Tandem Control IQ in children 2-5 years: TIR increases from 57% to 69%
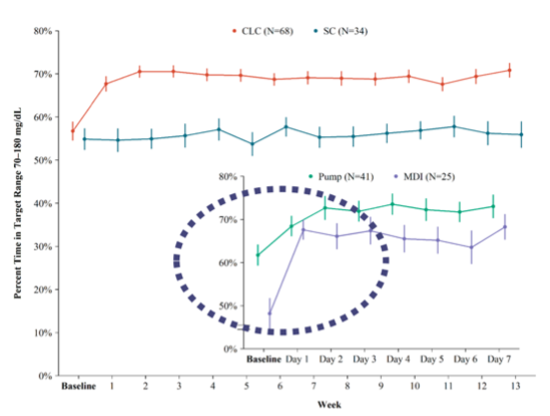
In the PEDAP study, 102 children (2-5 years) were randomized to Tandem Control IQ or standard care. Their baseline HbA1c was 7.6%.
Results after 13 weeks:
- In the group on Tandem Control IQ (n=68): TIR increased from 57% to 69%. The TBR remained stable at 3.1%.
- In the standard care (n=34): TIR increased from 55% to 56%. The TBR remained stable from 3.0% to 3.5%.
These data will likely be used to obtain approval for Tandem Control IQ in children aged 2-5 years.
A sub-analysis was also done within the group that started with the Tandem Control IQ:
- In the group that was previously on insulin pens (=25), the TIR increased from <50% to >70%. This is an increase in TIR of almost 20%!
- In the group that wore an insulin pump beforehand (n=41), the benefit was less spectacular, but still good.
The effects were always visible within the first days after starting the Tandem Control IQ system.
#2 MiniMed 780G in children 2-5 years: TIR increases from 58% to 66%
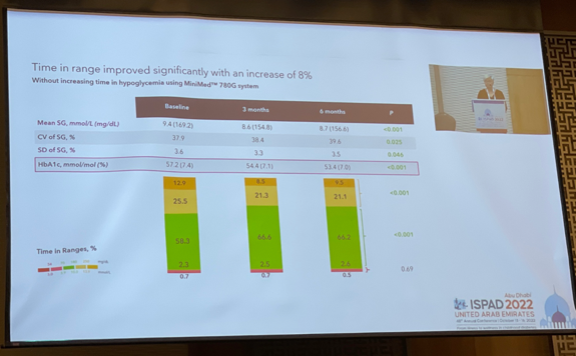
In a prospective study the MiniMed 780G was started in 35 children (2-5 years). Their baseline HbA1c was 7.4%.
=> After 3 months their TIR increased from 58% to 66%, and this remained stable after 6 months. The TBR remained stable (from 2.3% to 2.6%).
In this study, the children first used the MiniMed 780G in manual mode for 2 weeks before switching to auto mode,
and usually used the target value of 120 mg/dl, for fear of hypoglycemia in these very small children.
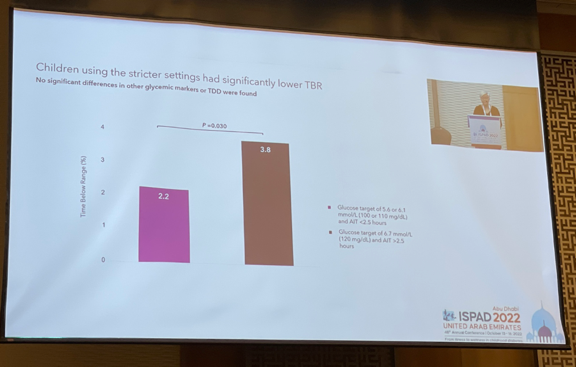
Strangely enough, using these less strict settings did not result in less hypoglycemia.
In fact, an association was shown between using stricter settings (the "ideal" target of 100 mg/dl and active insulin time of 2 hours) and less hypoglycemia.
I can't explain this very well.
CareLink data on >12000 people who used the MiniMed 780G in 2021 showed instead an association between less hypoglycemia at the less strict target value of 120 mg/dl.

3. Open-source closed-loop systems are "still in the game"
Several reviews of scientific data on commercial closed-loop systems have been published in recent months (such as this review and in this consensus), but these have focused less on open-source closed loop systems.
At the ISPAD, Dr. Petruzelkova (Czech Republic) now also gave an impressive overview of the scientific evidence surrounding open-source closed-loop systems (click on the figure for the PDF).

This scientific data proves the security and efficiency of open-source AID systems.
And just like with the commercial closed-loop systems, the development of the open-source closed-loop systems does not stop.
ISPAD gave a glimpse of the Pancreas4ALL study, which examines whether it is possible to use AndroidAPS as a fully closed-loop system.
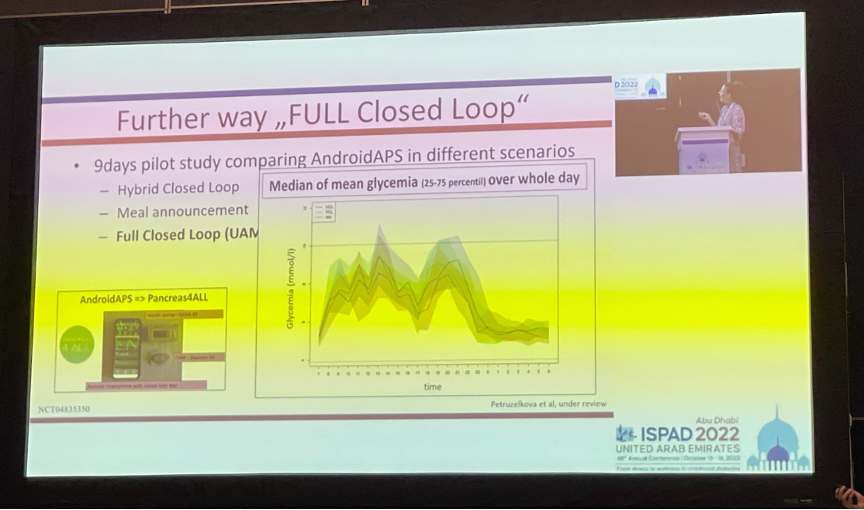
In this prospective study, the AndroidAPS algorithm is tested in 3 ways in 16 people with type 1 diabetes:
- in "hybrid closed loop" (i.e. entering boluses based on carbohydrate counting)
- in "closed loop meal announcement" (i.e. entering boluses based on meal announcements)
- and in "full closed loop" (i.e. without entering boluses with the function UAM - UnAnnounced Meal)
The study would be ready to be published, and the glycemic results between the 1st and 2nd groups should already have been similar.
In this article you can read how to use the MiniMed 780G in a more simple way and what the results are of the MiniMed 780G and Tandem Control IQ in very young children. You also got an overview of the scientific studies on open-source closed-loop systems and some hope that we can evolve to a fully closed-loop system in the near future.
If you would like to take a closer look at the differences between the main closed-loop systems, click here to download the "Overview of the 10 Best Closed-loop Systems".
Kind regards,
![]()